

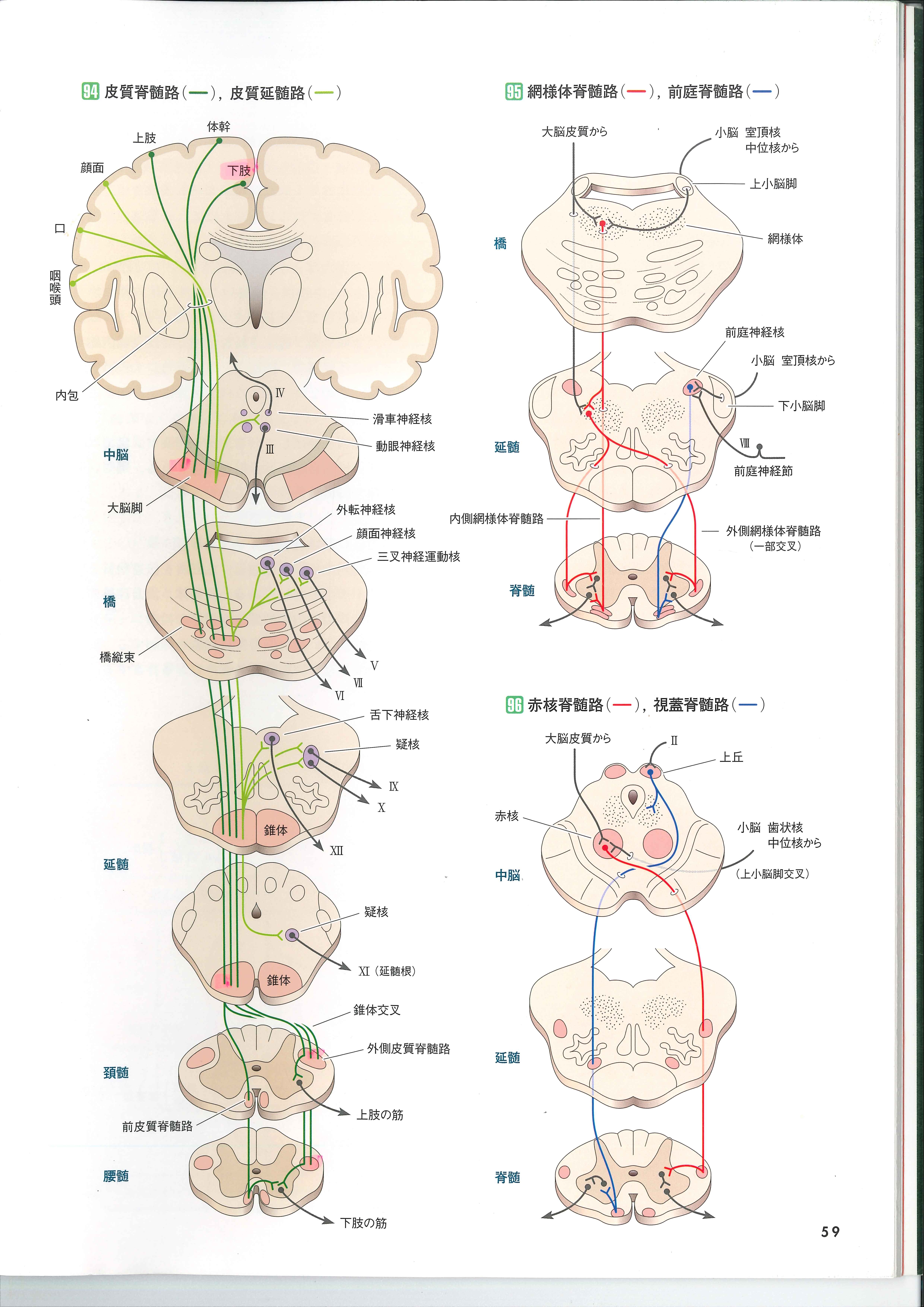
Here we talk about the way motor nerves travel from the cerebral cortex through the medulla oblongata or spinal cord. There are six. As explained in the Chapter "Movement mechanism", from the motor area of ??the cerebral cortex,
The lateral corticospinal tract (cortex-> spinal cord ) and the rubrospinal tract(red nucleus-> spinal cord ) mainly control the distal muscles of the extremities.
The?reticulospinal tract (reticular-> spinal cord ) ,?vestibulospinal tract? (vestibular nucleus- > spinal cord ) and ?tectospinal tract? (optic tectum- > spinal cord ) mainly involve trunk muscles and proximal limb muscles.
There are two things that control the distal extremities, the muscles around the limbs.They are the lateral corticospinal tract and the rubrospinal tract. It is the?reticulospinal tract , the vestibulospinal tract, and tectospinal tract that control the muscles of the proximal limbs, that is, the muscles that are attached to the trunk and the muscles of the trunk.
corticobulbar tract (cortex-> medulla oblongata ) leads to kinesthesia in cranial nerve and controls head and face movements.
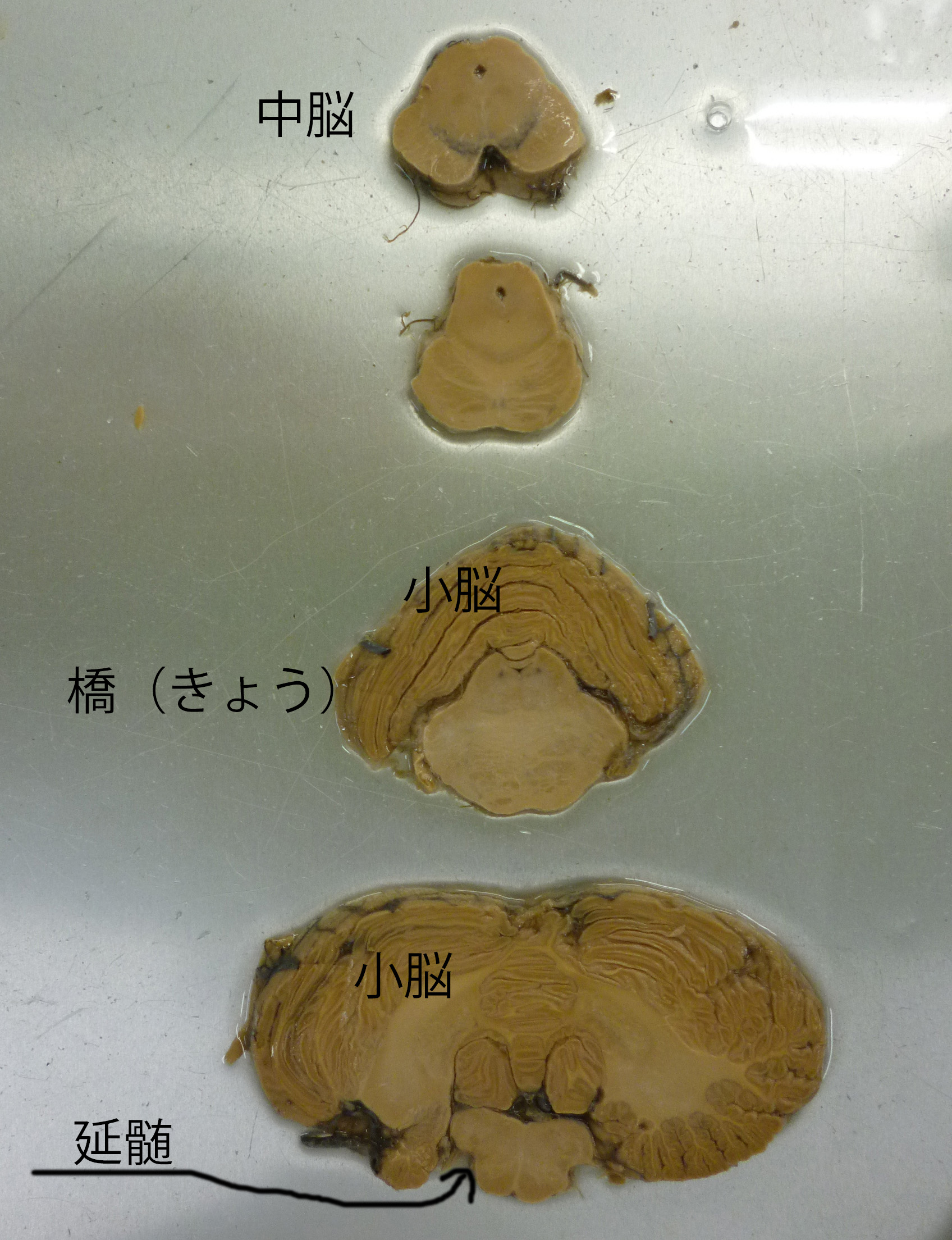
The picture below is taken from "Structure and Function Of Human Body".。
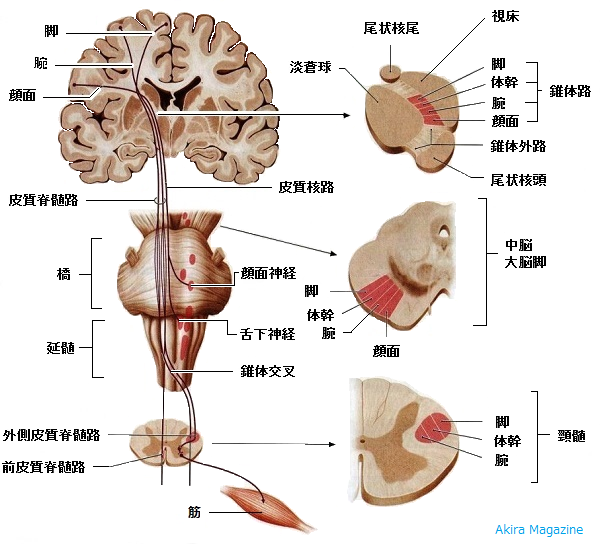
When the brain get injured from the outside till the cervical spinal cord, which muscles in the upper or lower limbs are initially immobilized? The answer would be lower limbs. Look at the picture above.
You can't see entire image just by the picure above.Therefore, we show anatomy from the cerebral cortex to the midbrain, pons, medulla oblongata and spinal cord.
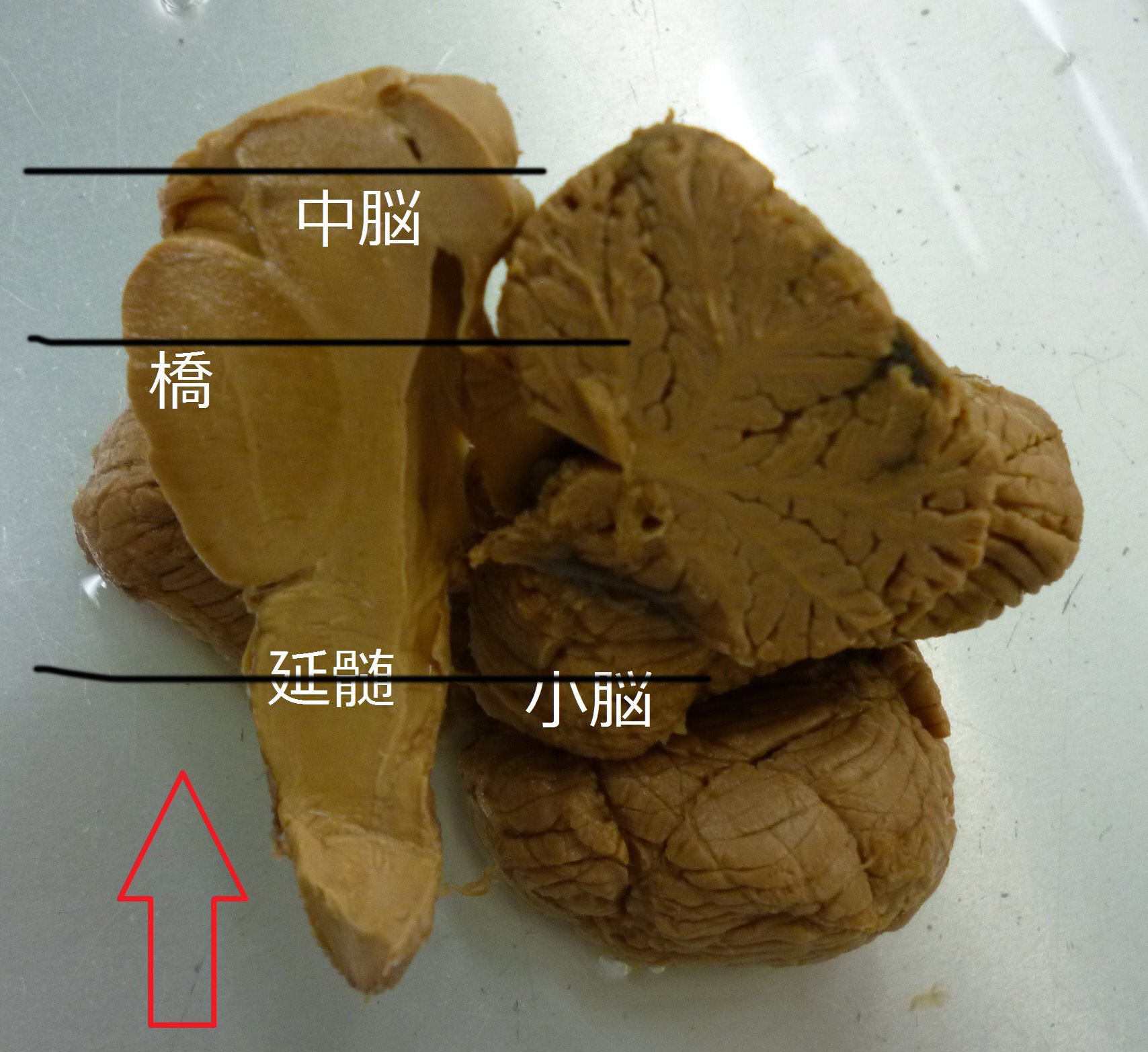
The picture above is a specimen from the anatomy.When it is sliced ??at the black line, and seen from the bottom like the red arrow,they are like the picture above it. Similarly, samples, cut horizontally, are shown below.
I tried moving this with an animation.
From the inside to the outside of the motor area of ??the cerebral cortex, innervation is distributed in order from lower limb, trunk, and to upper limb. The "corticospinal tract" is the largest descending path in the brain and transmits motor commands of the cerebral cortex to the spinal cord. It is also called the pyramidal tract because it passes through pyramid of medulla oblongata.It is new phylogenetically , emerged in mammals first and is most developed in humans.
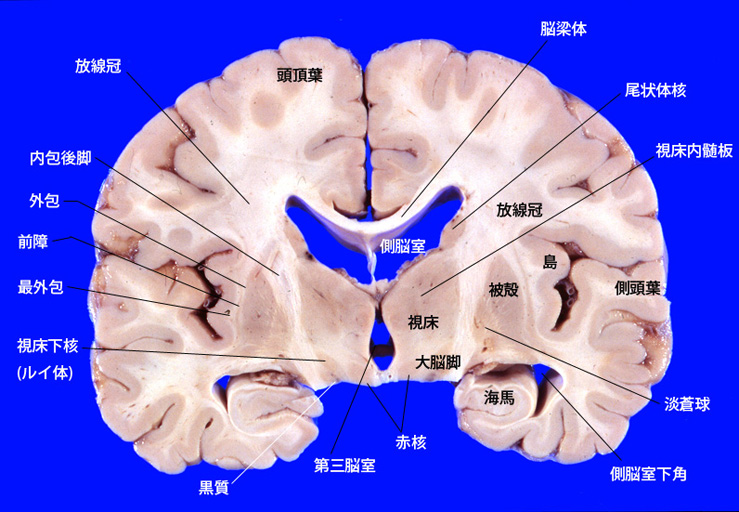
Cell of origin (pyramidal neurons) in the cerebral cortex are in the fifth layer of the cortex. The axons that extend from here form the coronary cortexcorona radiata, pass through posterior limb of internal capsule, and reach the midbrain. In the midbrain, it passes through the cerebral crus, splits into small bundles in the pon, and pass between the nucleus pontis. In the medulla oblongata, they join together again into a bundle to form?pyramid.
The animation below shows the nerve from the cortex to the cerebral crus. Please look slowly.
75% of the fibers cross the midline and migrate to the opposite side at a?pyramid the transition of the medulla oblongata and spinal cord. This movement is called pyramidal decussation. This tract is called the lateral corticospinal tract. It mainly regulates the movement of distal muscles. The remaining 25% of the fibers do not cross and this tract is called the ventral pyramidal tract. This spinal tract extends on both sides without crossing. It seems to regulate primarily the trunk muscles and the proximal muscles of the extremities.
The “rubrospinal tract” also regulates the same area as the corticospinal tract. It immediately crosses over from the red nucleus of the midbrain. The red nucleus is a pair of left and right nerve nuclei. It connects fibers from the motor area of ??the cerebrum and the cerebellar nucleus. Like the lateral corticospinal tract, it is involved in the distal muscles of the extremities and acts on the flexor muscles that cause joint flexion.
In the animation on the left, you can see the nerves that move the legs and the hands. This is the corticospinal tract.
The animation on the right represents the rubrospinal tract.
This spinal cord route is not just a link between the primary motor cortex and motor neurons in the spinal cord. In addition to the primary motor cortex,higher-order motor related areas(6 cortex), somatosensory cortex (3,1,2 cortex), 5 cortex also has nerves to the pyramid. It is distributed at a rate of about 30% each. These pyramidal neurons do not necessarily directly connect synaptic with motor neurons in the spinal cord.Some of them connect with?interneuron in the spinal cord. Direct synaptic connection seems to be involved in movement of the finger area.
Direct synaptic connection is shown in the figure below.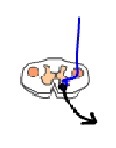
An interneuron is another neuron between neurons.

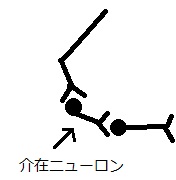
As shown in the animation, it is known now that not only single-line nerves (axons) extend to motor neurons, but they are entangled with interneurons in the spinal cord.
The animation goes back and forth, but,?you can see a?corticobulbar tract in the animation on the left above shown by the green line.
Fibers from the areas of the face, mouth, and pharynx outside?the?motor cortex, go through the genu of internal capsule, have direct synaptic connection to the motor neurons of the trigeminal nucleus of the brainstem, the facial nucleus, and the hypoglossal nucleus. Most of them are crossing in the brainstem.
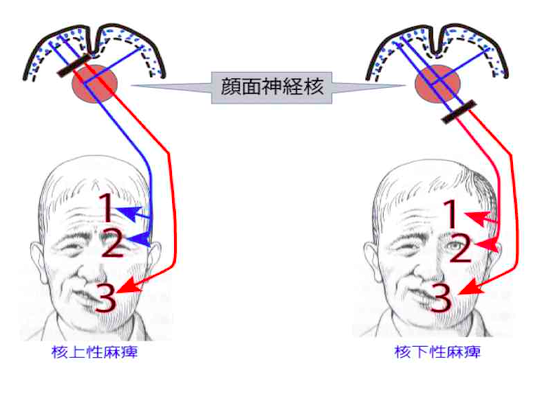
The way between the motor cortex of the cerebral cortex and facial nucleus is special.
Similar amount of fibers are flowing from the motor areas on both sides to the motor neurons that control the muscles of the upper part of the face.?The muscles of the lower part of the face is contoroled by the nerves from the motor cortex on the opposite side. Therefore, when one cortical medullary tract is damaged, the eyebrows and eyelids are normal, the mouth does not move, and descends as shown in the left face painting.?Supranuclear palsy occurs when the upper part of the nucleus is damaged.
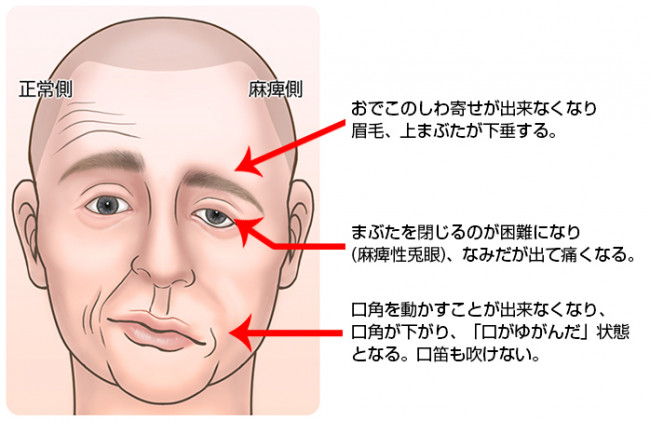
In the case ofinfranuclear palsy, all the nerves don't work, so the forehead cannot be wrinkled, the eyelids do not close, and the corners of the mouth drop, as in the picture on the right below.?
It may be confusing, but here we show the reticulospinal tract (reticular-> spinal cord) , vestibulospinal tract (vestibular nucleus-> spinal cord). These nerve tracts control the trunk muscles and the proximal muscles of the extremities.
When the corticospinal tract is damaged somewhere along the motor cortex pathway from the motor cortex,three of symotom below appear.
Motor paralysis
accentuation of tendon reflex
Appearance of abnormal reflections such as the Babinski reflection
Motor paralysis means that when a motor neuron is cut off, the muscle cannot move because the stimulus is not transmitted to it.
The description about Babinski reflex is shown below( quote from http://in-and-out.lolipop.jp/?p=2101)
Babinski discovered it.
According to the record, Mr. Babinski was scratching around the patient's leg sleeping in bed in turn instead of saying hello. He found that most people bend their big toes, while some bend back.
28 lines This published paper is 28 lines long and is said to be a nice and concis,which cannot be deleted any more.
"On the plantar skin reflex in some organic diseases affecting the central nervous system"
J. Babansky (From a report of the Biological Society held on February 22, 1896)
Abnormal plantar skin reflexes in a significant number of patients with hemiplegia or monoplegia of the lower extremities due to organic disorders of the central nervous system.
Poke the sole with a needle, and on the non-paralyzed side, flex the thigh to the pelvis and the lower leg to the thigh, the foot to the lower leg, and the toe to the metatarsal bone as would normally be seen in a normal person.
When the same stimulus was applied on the paralyzed side, flextion of thigh, lower leg and foot was the same as the non-paralyzed one, but the toes stretched to the metatarsal bone instead of flexing.
Such reflex are observed in both patients who havehemiplegic for only a few days, and patients who have spastic hemiplegicfor several months.Also,it is seen in both patients who cannot voluntarily move their toes and who still can. However, it should be added that such anomalies are not always seen.
The toe extension movement that occurred when the sole of the foot was poke was also observed in some cases of paraplegia due to an structural disorder of the spinal cord. However, in such cases, the actual condition of the abnormality is not so obvious because there is no comparative part.
In summary, speaking about reflex movements caused by plantar needle stimulation to the patients with lower limb paralysis from structual disorders of the central nervous system, as is already known, not only the intensity of reflection changes, but also the form of reflection becomes abnormal.
Why does it happen?

Image quoted from :バビンスキー反射 ? Wikipedia
The Babinski reflex reported in this way is widely known for its evaluation method and phenomenon.
Why does it occur? I would like a physiological explanation if possible.
I ended up in the literature of Dr. Yasuo Toyokura, who reported the Babinski reflex.He became a professor at Tokyo University in 1964, contributed much to medical profession by discovering the etiology of SMON and coining the word "neurology".
Mr. Toyokura's commentary on Babinski reflection
There has been much debate about the appearance of the Babinski reflex. It is generally classified as a multisynaptic superficial reflex, and it is said that part of the lower limb flexion reflex to noxious stimuli appears. What should be noted is the force relationship between the plantar flexors and dorsiflexors. When the sole of the foot is stimulated, it changes depending on the location and strength, but it stimulates both muscle groups. Here, in the healthy person, the plantar flexor muscle group contracts more strongly, but in patients with pyramidal tract disorders, the threshold of the dorsiflexor group is significantly lower, and the toes are extended. This has been revealed by EMG studies. Then why is the plantar flexor group usually significant? This is explained in the hypothesis from Dr. Toyokura in easy way. The following is a quote.
As an interpretation of this, it is important to consider the developmental history of the dorsiflexor group of the foot and the anthropological consideration of human's acquisition of erect bipedalism.
In the process from the infant to the erect bipedalism of the adult, the kicking (plantar flexion) movement of the foot, which the infant does not have, is further strengthened. In addition, in the foot that has been able to support the weight by erect bipedalism, the mobility of the foot limb are significantly limited, and the mobility other than plantar and dorsiflexion is almost disappered. This is in contrast to the marked mobility of the fingers.
In other words, strengthening of the plantar flexor muscles of the foot in adults should be regarded as an important developmental process both individual and phylogenetically. This suggests that the plantar reflexes is storongly shown in?plantar muscle reflex in the normal adult.
In addition, the Babinski reflex is a reflex that can be seen only in humans except some apes, and in humans there is no reflex similar to the Babinski reflex in the upper limbs. For thinking about this, it is not evitable to consider the significant differentiation of the lower limbs and upper limbs in human history.
Please click the URL below and watch the video. The right foot has a positive Babinski reflex. The thumb is warped. The left foot is negative. That is normal.
https://www.youtube.com/watch?v=ZFu7bdbnZx8
Infants will have a positive Babinski reflex. In other words, if you rub the sole of your foot from your heel to your little finger and rub it with a toothpick,the thumb will bend back and the other four fingers will open like a fan. This is normal.
https://www.youtube.com/watch?v=EoutYFC0Nss
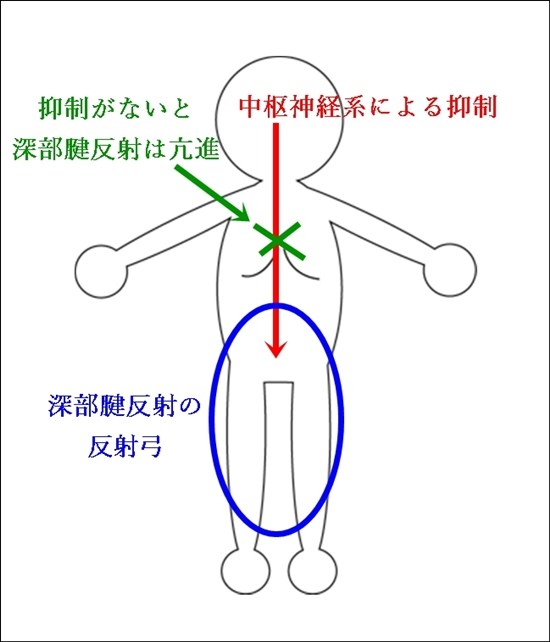
Next, I would like to talk about the enhanced tendon reflex . In the pyramidal tract disorder, the patellar reflex is strongly manifested. This reflex is seen under normal conditions. The mechanism is as follows.
There are two kind of reflex ;a single synaptic reflex in which a afferent fiber, which is an input from the demand, is immediately connected to an output neuron only via one synapse and a multi-synaptic reflex that is connected to an output neuron via multiple synapses.
The stretch reflex is known as an example of the monosynaptic reflex. The stretch reflex is a reflex that receives a stretch of a muscle as a stimulus, and contracts the muscle to keep the length of the muscle constant
The patellar reflex is famous as a typical example of the stretch reflex. Quoted from
http://tsunepi.hatenablog.com/entry/20130731/1375270286

The components of the?reflex arc of the patellar tendon reflex are
Receptor: Muscle Spindle in quadriceps muscle
Afferent pathway: Femoral nerve
Reflex center: α motor neuron of anterior horn
Efferent pathway: Femoral nerve (α motor fiber)
Effector: Quadriceps muscle
Hitting the quadriceps tendon under the patella will stretch the quadriceps.
When a muscle is stretched, the muscle spindle contained in it also stretches. Receptor potentials are generated by the extension of the muscle spindle.
・Significance of patellar tendon reflex
The stretch reflex is prominent in the muscles that support the body against gravity (antigravity muscles), which means that it plays an important role in maintaining human posture. In addition, for example, when landing by jumping, the quadriceps muscle contracts due to reflexes, which also has the effect of reducing the burden on the body. As shown in the picture below, the patellar tendon reflex hardly respond by a central command.
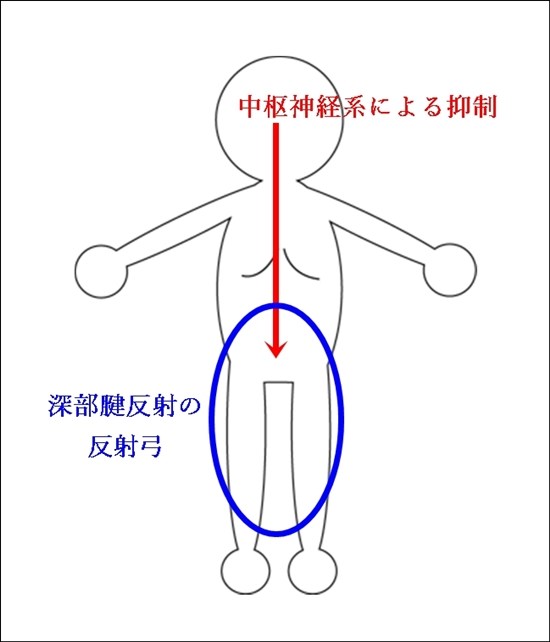
A central disorder results in loss of central depression and increased tendon reflexes.?This is called brisk reflex.
The URL below is a video with enhanced patellar tendon reflexes. It is the result of a central nervous system impairment. 。
https://www.youtube.com/watch?v=lauwuPX0j_M
The presence of motor paralysis, enhanced tendon reflexes, and abnormal reflexes such as the Babinski reflex are called pyramidal tract symptoms.
On the other hand, movement disorders associated with involuntary movements (abnormal movements that occur regardless of one's will), abnormal muscle tone, rather than motor paralysis, have been called extrapyramidal symptoms. It was mainly considered to be a lesion of the basal ganglia and was considered to be independent of the?corticocerebral motor area.
Nowadays, it has been found that there is a tight connection of nerve fibers between the motor cortex and the basal ganglia, and there is no extrapyramidal system that controls the descending path besides the pyramidal tract.However the distinction between pyramidal and extrapyramidal symptoms is diagnostically important and words remain.
Let's talk about sense.
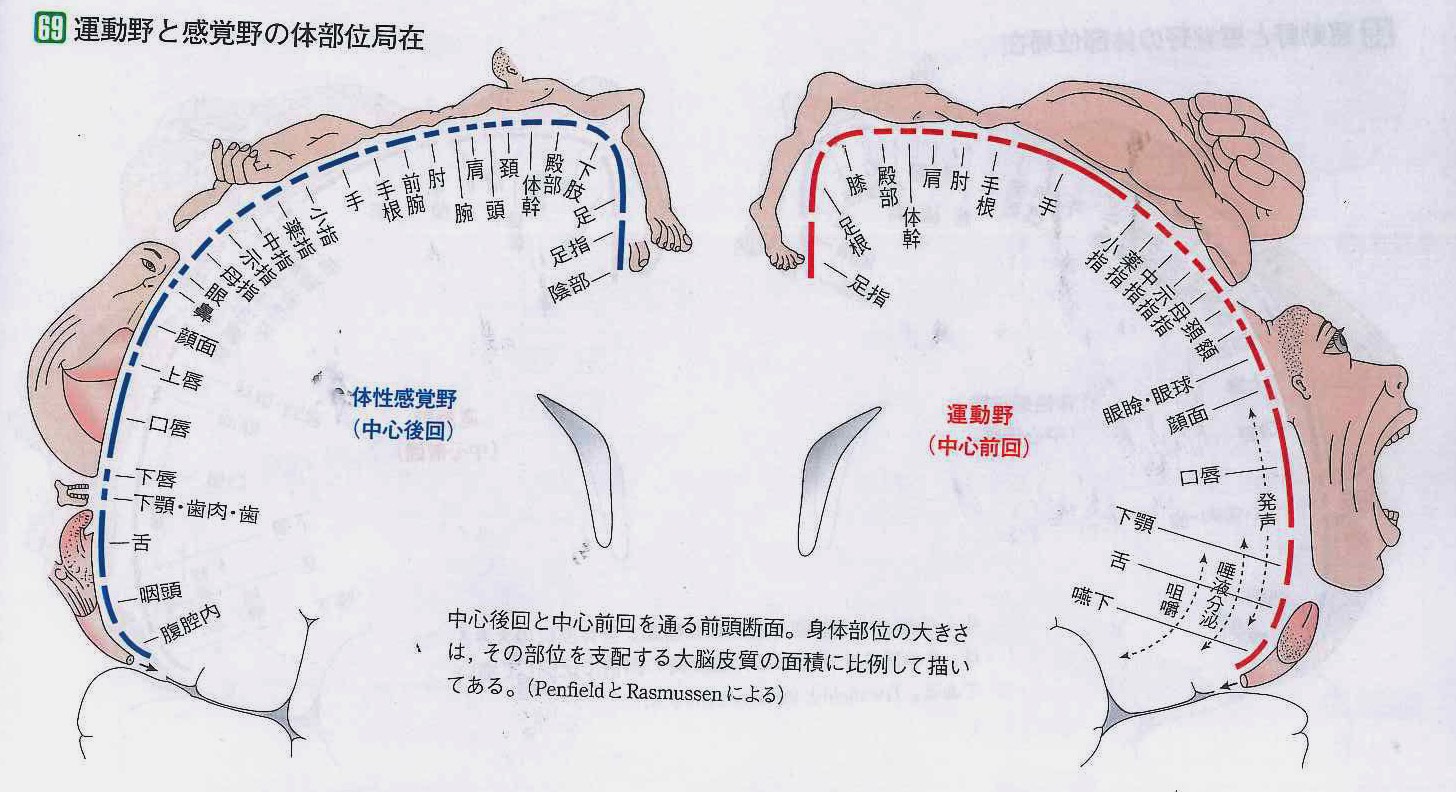
As shown in the picture on the left, the somatosensory area gets sensation nerves from the limbs, face, and trunk. The face is drawn large,and the feeling nerves from the hands and face occupies larger area in the cerebral cortex than the one from the feet.This means that your nerves are distributed to the end of your hands and face.
Stimulation of the senses from the hands, feet, goes through the spinal cord and reaches the brain cortex. The senses is roughly classified into sense of warmth,?algesia, tactile sensation, and bathyesthesia. The sense of the face and head which is the 5th cranial nerve (trigeminal nerve) enter the trigeminal nucleus. After that, it moves to the thalamus on the other side and to the?somatosensory area shown in the right picture.
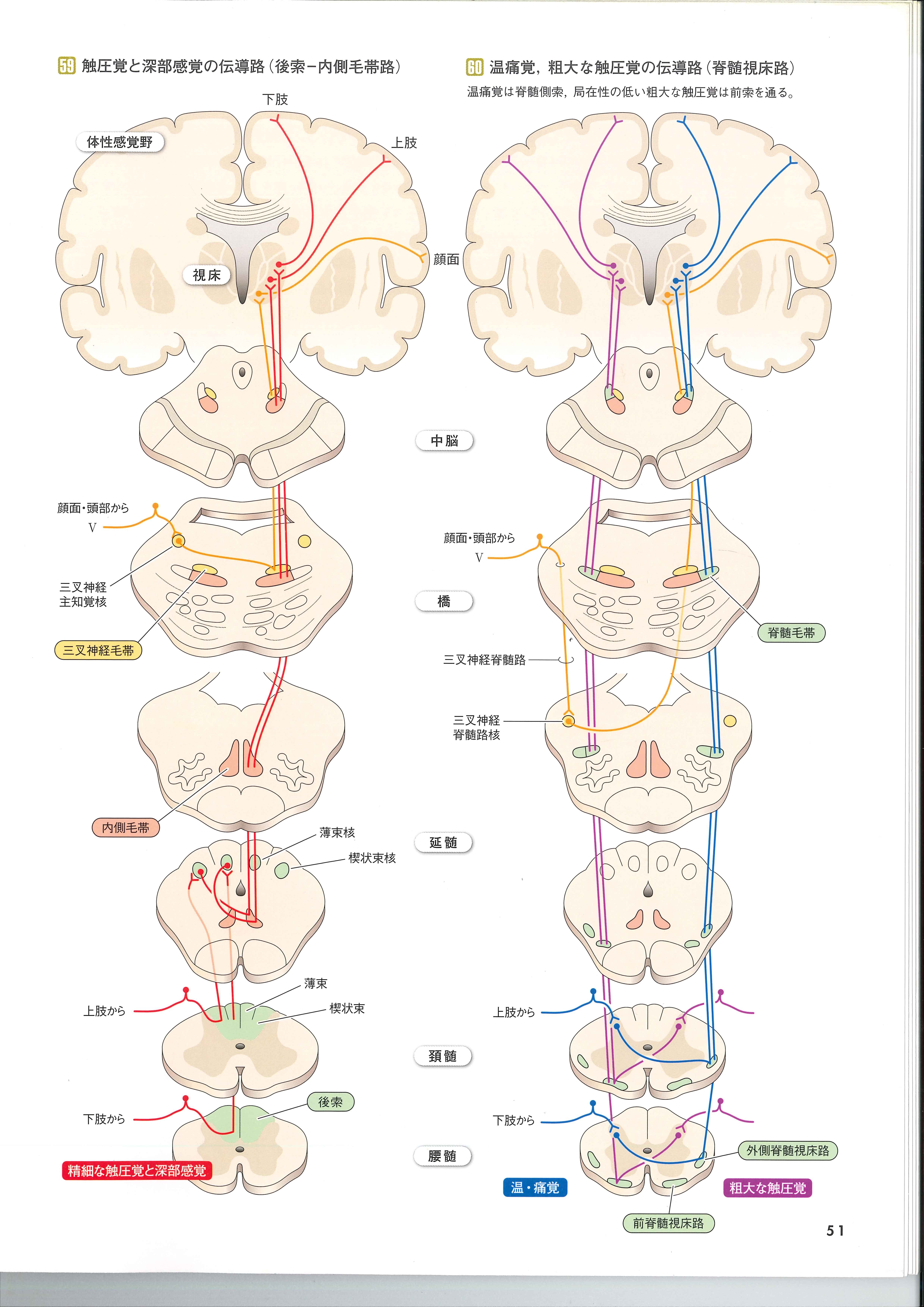
See the flow of each sensory nerve in the picture below.
First of all, sense of warmth,?algesia, rough tactile sensation pass through the nerve paths of the lateral spinal thalamus and anterior spinal thalamus , as shown in the picture below. Fine tactile sensation and bathyesthesia move from the dorsal cord to the medial lemniscus.
The sense of warmth,?algesia, rough tactile sensation follow the nerve pathways of the lateral spinothalamic tract and?anterior spinothalamic tract. Fine tactile sensations and bathyesthesia pass through the dorsal cord to the medial lemniscus. |
The sensory nerves transmit the stimulation of the senses to the sensory area on the opposite side. Therefore, if the cerebrum is damaged due to a disease of the brain, the sense on the other side becomes abnormal.
Quoted from normal structure and function of human body VIII (nerve system)
I tried to see this nerve flow in animation.

When the spinal cord is injured from below the cervical spinal cord, the sensation is lost in the order of foot, trunk and hand.
The movement also is restricted in order from foot to hand.
About the spinal cord
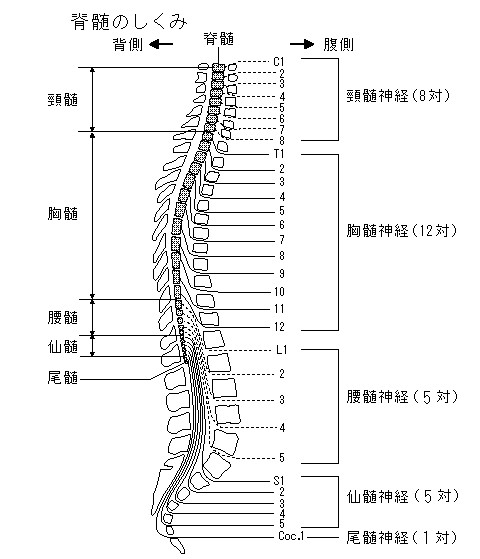
As shown in the figure on the right, the space surrounded by the bones of the spine and containing the spinal cord is called the spinal canal. It's like a clay pipe.The spinal cord is inside it.
The relationship between the spinal cord, spinal canal and spine is shown in the animation below. The 8th week of gestation is when fetus is in mother's belly. The spine grows from newborn babies to adults.
On the other hand, the spinal cord does not grow. the ends of the spinal cord in the spinal canal gradually become thinner.
The ends of the spinal cord comes till about the second lumbar spine when we are adults. Whiile we are children, as the spine extends, the spinal cord is left behind below the second lumbar spine.
Next let's see an overview of the area around the spinal cord.
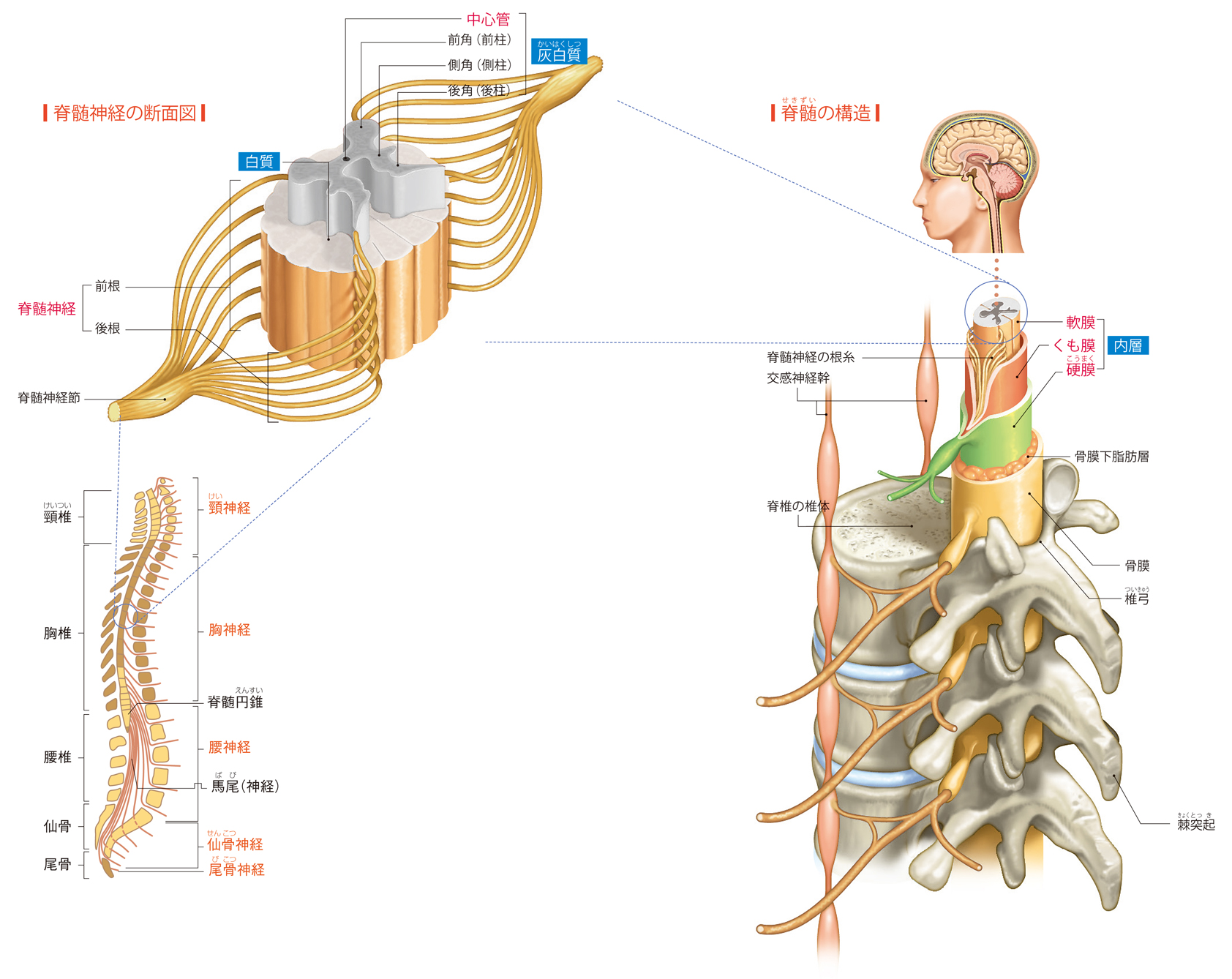
From the picture below,you can see the nerve named anterior root which connects front of spinal cord and the nerve named posterior root which connects back of the spinal cord From behind, sensory nerves enter the spinal cord. From the front, motor nerves goes out from spinal cord.This will always be like this.
Quoted from https://health.goo.ne.jp/medical/body/zukan/8/article-6.html
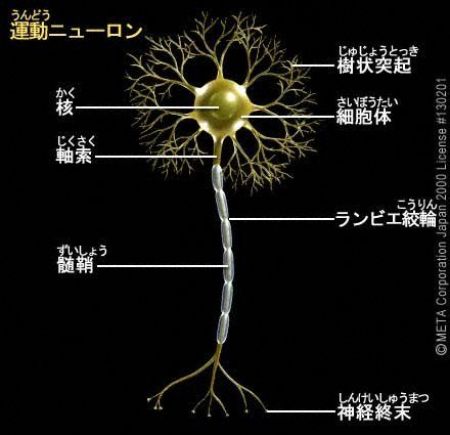
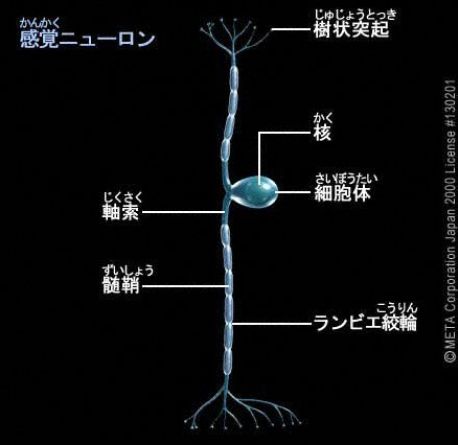
Sensory nerves and motor nerves have different shapes.
Quoted from https://kotobank.jp/word/%E7%A5%9E%E7%B5%8C-81577
Quoted from http://comedical.blog23.fc2.com/blog-entry-752.html
http://manabu-biology.com/archives/40113558.html
In the cross section of the spinal nerve,
There is the spinal ganglion in the sensory nerves. Look at the picture. This is where the upper sensory nerve cell bodies are clustered. Because the cell bodies gather, they are slightly swollen. Let's see this in anime.
Next, let's look at the motor nerves.
I will show the anatomy of the spinal cord. There are various names.
This side is the back side of the body
The front side of the body
Next, is the spinal cord similar in structure everywhere?The answer is No.
In the cervical ampulla which has the 7th cervical cord ,and the?lumbar ampulla, which has the 4th lumbar cord, there are many motor neurons distributed in the limbs, so the anterior horn is developed.
In the chest where the second thoracic spinal cord lies, there are a lot of preganglionic sympathetic neuron distributed in the organ, so the lateral horn are developed.
The white matter where nerve fibers located outside the spinal cord occupies a larger area toward the head. This is because the nerve fibers from the limbs and trunk increase.
The area of ??the 3rd sacral region of spinal cord is small because there are few nerve fibers.
Sensory nerves that enter the spinal cord and motor nerves that exit from the same place of spinal cord connct to the same muscle and skin.
This area of ??skin is called the dermatome. The boundaries are unclear and is distinguished approximately.
The area where the motor nerves dominate is called the myotome.
The human body is divided into 31 sections from each spinal nerve, the dermatome and the myotome.
When a human touches something and have a sensation (hot, cold, pain, etc.), a signal is sent to the spinal cord that controls the dermatome, and the brain recognizes it.
On the contrary, when a human want to move the part of the body, a signal is sent from the brain to the spinal cord that controls the myotome, and the body moves.
The nerves of dermatome and myotome are different, but since they come from the same spinal cord, the extent of the area is almost the same.
This is shown in the figure.
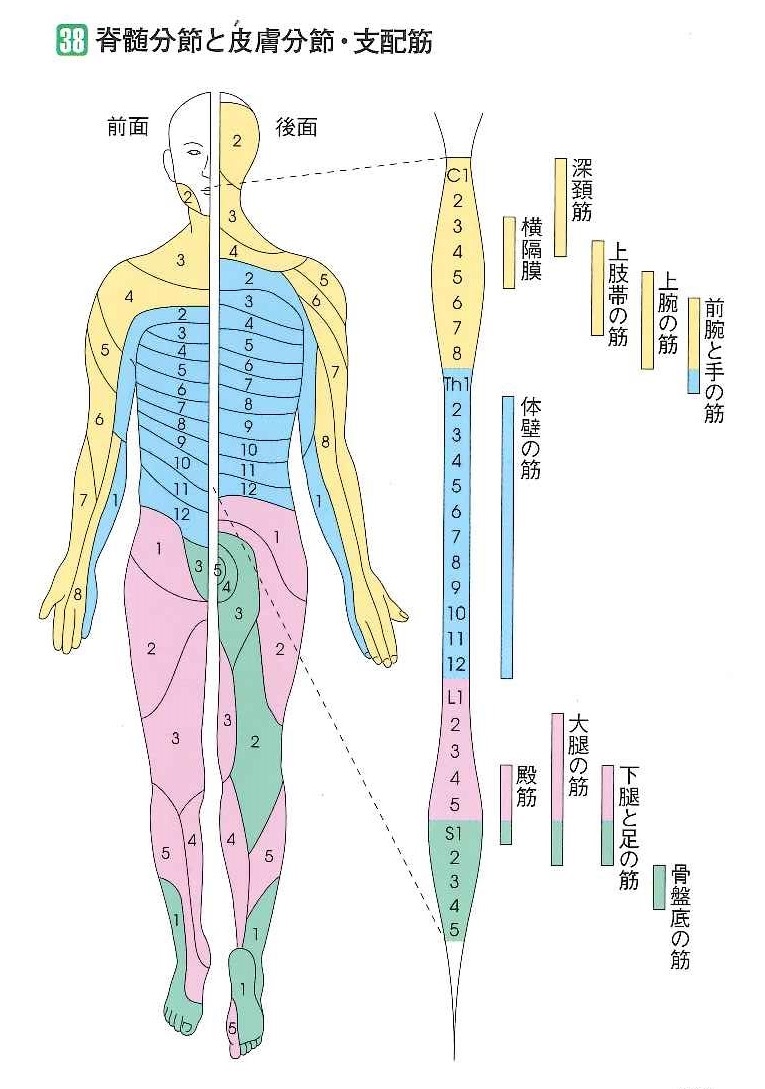
There are 8 pairs of sensory and motor nerves coming out of the cervical spine.
For example, the nerves that control the diaphragm are #3 ,#4 and #5 of the cervical nerves.
The sensory and motor nerves of the trunk are #2 to #12 in the ?thoracic vertebrae.
If a human have pain in paticular part of the body or cannot move the area,the damage of the skin surface area, the spinal cord itself, or the spinal nerves coming from spinal cord are considarable.